정신약물의 처방이 많아질수록 자살이 많아진다- 논문
페이지 정보

본문
몇개의 연구결과 나타난 증거에 의하면 정신건강 정책과 정신의료서비스에 돈을 더 많이 쓰는 사회, 즉 정신약물의 처방이 많아질수록 자살이 많아진다는 내용입니다
심리부검은 자살자 본인이 아닌 주변 인물에 대한 질문을 통해 행해 지는데 그 질문내용을 분석하면 자살을 정신질환과 연결시키는 내용으로 신빙성이 없다는 비판의 논문-(권오용 KIMI사무총장)
Evidence That More Psychiatry Means More Suicide

Maria Bradshaw
January 12, 2014
This has got to stop. Around the world a million people die from suicide each year and the response internationally is to pour more funding and channel more people into psychiatric services. Three large studies have now found that the more we spend on mental health services the higher our suicide rates. In addition, a recent study has completely discredited claims that 90% of those who die from suicide are mentally ill at the time of their death. We need to use this evidence to stop the expansion of psychiatry as a suicide prevention measure.
In 2004 a group of Australian researchers and the WHO conducted a studyacross 100 countrieswhichtested the theory that the implementation of national mental health policies,programs and legislation would be associated with lower national suicide rates. They found the opposite.
The introduction of a mental health policy and mental health legislation was associated with an increase in male and total suicide rates, and the introduction of a therapeutic drugs policy was associated with an increase in total suicide rates.[1]
The authors were bemused. Given their belief that mental illness causes suicide, they found the results counter-intuitive and rushed to dismiss them. It would be naïve, they said to accept the findings without question. They stated that there was a clear need for further studies in the area.
And so another study was done.
In 2010 researchers from the UK replicated the results and found suicide rates were increased in countries with mental health legislation, higher spending on mental health, greater numbers of psychiatric beds, psychiatrists and psychiatric nurses, and the availability of training in mental health for primary care professionals.[2]
As with the previous study, the authors cautioned against accepting their findings and advised that further studies were needed to replicate the results of their study.
Recently a third, much larger, study was conducted over 191 countries and a population of 6.4 billion people. This study controlled extensively for economic factors and found that numbers of psychiatrists and mental health beds were significantly positively associated with population suicide rates and concluded that “Countries with better psychiatric services experience higher suicide rates.”[3]
The authors are again cautious about their results but note that their study corroborates the positive associations between mental health provision and population suicide rates and suggest that “The consistency of these findings indicates the need to examine potential underlying pathways.”
What makes these authors so ready to question their findings and suggest they be treated with caution? It is, I think, the ubiquitous belief that suicide is caused by mental illness. The 2004 study states
It would be anticipated that cohesive, national mental health strategies would be associated with comparatively low suicide rates, given that mental health problems significantly increase the risk of suicide.
The 2010 study states
Availability of healthcare services may reduce suicide rates by allowing identification and treatment of mental illness.
And while the most recent study takes a more skeptical approach to the notion that mental illness causes suicide and psychiatric treatment reduces it, it does not directly challenge the data on which the links between suicide and psychiatric illness are made.
While data from high income countries indicate that severe psychiatric illnesses, especially depressive disorders, are the principal cause of suicide, research from LMICs (Low to Medium Income Countries) suggests that social, economic and cultural factors also have significant influence.
This idea that psychiatric disorders are present in over 90% of suicides is based on psychological autopsies, not on data about diagnosis before death. In a psychological autopsy, dead people are labelled with psychiatric diagnoses on the basis of interviews interviewing a few of the relatives and/or friends.
I have spent five years arguing that psychological autopsies have no reliability or validity and that the idea that almost every suicide can be explained as a product of mental illness is a marketing message not a scientific finding. The issues associated with diagnosing a living person are well known – how many more issues must exist in performing a psychiatric assessment on someone who is dead?
The authors of my new favourite study introduce their work with the claim that
One of the most established “truths” in suicidology is that almost all (90% or more) of those who kill themselves suffer from one or more mental disorders, and a causal link between the two is implied. However, there has been little reflection on the reliability and validity of this method.[4]
They challenge the reliability of the psychological autopsy process on numerous grounds. They argue, for example, that some questions in a diagnostic interview are impossible for someone other than the subject of the question to answer, and ask “is it really possible to assign psychiatric diagnoses to someone who is dead by interviewing someone else?”
What living person would be happy to be diagnosed as depressed on the basis of their mother/brother/friend (a proxy) answering the following questions about them?
- In the last month, did you lose interest or pleasure in things you usually enjoyed?
- How did you feel about yourself?
- Did you have troubles thinking or concentrating?
- Were things so bad that you were thinking a lot about death or that you would be better off dead?
- If something good happens to you or someone tries to cheer you up, do you feel better at least for a while?
- Is your feeling of depression different from the kind of feeling you would get if someone close to you died?
- Have you been feeling guilty about things you have done or not done?
- Do your arms or legs often feel heavy (as though they were full of lead)?
- Are you especially sensitive to how others treat you?” “What happens to you when someone rejects, criticizes, or slights you?
- Have you avoided doing things or being with people because you were afraid of being criticized or rejected?
Is a spouse/parent/child able to reliably answer the following questions which may lead to a diagnosis of substance abuse disorder?
- Did you need to drink more in order to get the same effect that you got when you first started drinking?
- During the times when you drank alcohol, did you end up drinking more than you planned when you started?
- Have you tried to reduce or stop drinking alcohol but failed?
The researchers point out that “most questions asked to assign a diagnosis are impossible to answer reliably by proxies, and thus, one cannot validly make conclusions.”
While the authors of psychological autopsy studies claim the diagnostic tools they use are reliable and valid, they ignore the important fact that they have not been validated for use by proxies. The authors point out that family members or friends may have opinions about a dead person’s mood and drinking behaviour, but that such subjective opinions do not necessarily represent the reality of the deceased. They point out that “Proxies can speculate, but such speculations can hardly be used to assign psychiatric diagnoses to others.”
The study points to evidence from studies of suicide attempts showing that differences have been found between what the person who has made the attempt says about their mood, feelings and intentions and what his/her family or doctors say about them .
It questions the validity of psychological autopsies based on the fact that in assessing mood disorders some of the indicators are about suicidality. Given the person has already killed themselves they receive an automatic positive on this criterion and as such the threshold for diagnosis is lowered. Before the interview has commenced, then, suicide victims are more likely than controls to reach the diagnostic criteria and as such is an effective way of ensuring that the results show suicide victims are more mentally disordered than other groups of people.
As the diagnostic threshold for mental disorders is lowered with each new iteration of the DSM, more and more suicide victims will be retrospectively labelled mentally ill. For these and other reasons, the authors state that “as a diagnostic tool psychological autopsies should now be abandoned.”
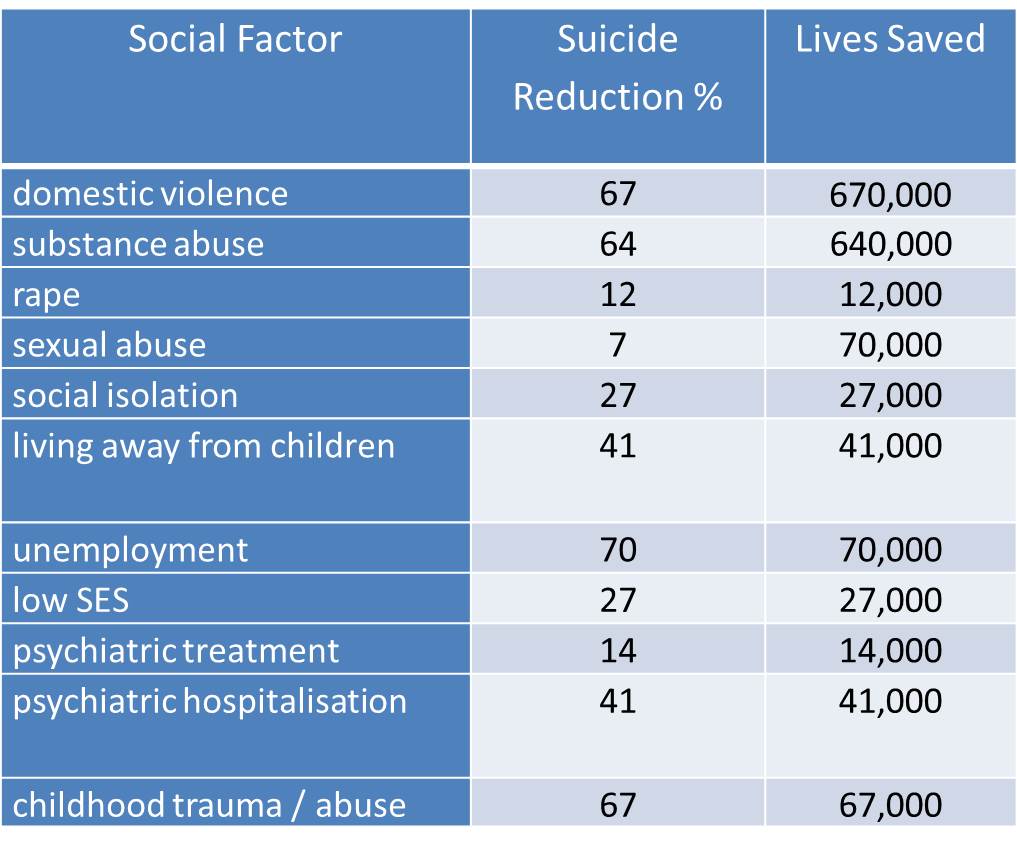
A range of social factors have been associated with suicide risk. The following table shows the percentage reduction in suicide that a variety of studies have estimated could be achieved through elimination of these factors, and based on WHO estimates that 1,000,000 people worldwide die from suicide each year, the number of lives that could be saved.
Spending on mental health treatment in the United States was $155 billion in 2009, with prescription drugs accounting for 29% of spending.[5] The State of California alone spending $1.842 billion in 2011-12[6]
In 2008, the OECD reported that a recent analysis had shown that 28 European countries had spent more than ?118 billion just on treatment for depression. This figure comprised direct costs of ?42 billion; ?22 billion for outpatient care, ?9 billion for pharmaceuticals and ?10 billion for hospitalisation, with indirect costs due to work absenteeism and premature mortality estimated at ?76 billion.[7]
Australia spent over $6.3 billion on mental health-related services in 2009–10, Ireland spent ?113m on psychiatric drugs in 2009[8] and England spent £1.1 billion on mental health services for people aged 18-64 in 2012.[9]
We spent all this money, and the more we spent the more our suicide rates increased. More people died – alone and in anguish – by their own hands. More families were destroyed and left to live with unimaginable pain and grief. Less money was available to address the real causes of emotional distress and suicide.
This has got to stop and I think it could if each one of us presented this data to our local government representative, spoke to our local media or called a meeting of voters in our community. A million people will take their lives in 2014 unless we join forces and use the data these researchers have provided us to make this stop. In this new year, do you think you could do something?
References:
[1] Philip Burgess, Jane Pirkis, Damien Jolley, Harvey Whiteford, Shekhar Saxena Do nations’ mental health policies, programs and legislation influence their suicide rates? An ecological study of 100 countries Australian and New Zealand Journal of Psychiatry 2004; 38:933–939
[2] Shah, Ajit ; Bhandarkar, Ritesh ; Bhatia, Gurleen The Relationship Between General Population Suicide Rates And Mental Health Funding, Service Provision And National Policy: A Cross-National Study International Journal Of Social Psychiatry Volume: 56 Issue: 4 Pages: 448-453 Doi: 10.1177/0020764009342384 Published: Jul 2010
[3] A.P. Rajkumar, E.M. Brinda, A.S. Duba, P. Thangadurai, K.S. Jacob National suicide rates and mental health system indicators: An ecological study of 191 countries International Journal of Law and Psychiatry 36 (2013) 339–342
[4] Heidi Hjelmeland Gudrun Dieserud Kari Dyregrov Birthe L. Knizek Antoon A. Leenaars Psychological Autopsy Studies As Diagnostic Tools: Are They Methodologically Flawed? Death Studies, 36: 605–626, 2012 Copyright Taylor & Francis Group, LLC http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3662079/pdf/udst36_605.pdf
[5] Substance Abuse and Mental Health Services Administration. (2013). Behavioral Health, United States, 2012. HHS Publication No. (SMA)13-4797. Rockville, MD: Substance Abuse and Mental Health Services Administration.
[6] State of California Mental Health Services Act Expenditure Report Fiscal Year 2013-14 http://www.dhcs.ca.gov/formsandpubs/Documents/Legislative%20Reports/Mental%20Health/MHSA_Expend_Report-Jan-2013.pdf
[7] ORGANISATION FOR ECONOMIC CO-OPERATION AND DEVELOPMENT Policy Brief NOVEMBER 2008 Mental Health in OECD Countries http://www.oecd.org/els/health-systems/41686440.pdf
[8] Irish Examiner 5m drug prescriptions for mental health a year Friday, August 05, 2011 http://www.irishexaminer.com/ireland/5m-drug-prescriptions-for-mental-health-a-year-163317.html
[9] Health & Social Care Information Centre Personal Social Services: Expenditure and Unit Costs, England – 2012-13, Provisional release [NS] Publication date: September 19, 2013 http://www.hscic.gov.uk/catalogue/PUB11644
출처:http://www.madinamerica.com/2014/01/evidence-that-more-psychiatry-means-more-suicide/
댓글목록
등록된 댓글이 없습니다.